How Oral Nutrient Absorption Actually Works
The oral route is the most common and convenient way to consume nutrients and bioactive compounds. However, oral intake does not guarantee effective absorption. The amount of a nutrient that ultimately reaches systemic circulation depends on multiple physiological and biochemical barriers within the gastrointestinal tract.
Understanding these barriers explains why many nutrients and bioactives show low oral bioavailability—and why formulation strategies play a critical role.
1. Why Oral Absorption Is Often Inefficient
Micronutrient deficiencies commonly involve iron, vitamin B12, calcium, magnesium, and fat-soluble vitamins, despite adequate intake. This is because oral absorption is influenced by:
• Limited solubility in gastrointestinal fluids
• Poor permeability across the intestinal wall
• Enzymatic degradation
• Efflux transport mechanisms
• First-pass metabolism in the liver
As a result, the absorbed dose is often significantly lower than the consumed dose.
2. Digestion and Absorption Along the Gastrointestinal Tract
After ingestion, food and formulations undergo:
• Mechanical processing in the mouth
• Chemical digestion in the stomach and small intestine
The small intestine (duodenum and jejunum) is the primary site of absorption, accounting for nearly 90% of nutrient and drug uptake, due to its large surface area created by villi and microvilli.
3. Carbohydrate Absorption and the Role of the Microbiome
Carbohydrate digestion begins in the mouth and continues in the intestine through enzymes secreted by the salivary glands, pancreas, and intestinal brush border.
Some carbohydrates, such as dietary fiber, resist digestion and pass into the colon, where they are fermented by gut microbiota. This fermentation produces short-chain fatty acids (SCFAs) that support gut health and metabolic regulation, highlighting the indirect role of the microbiome in nutrient utilization.
4. Protein Digestion and Enzymatic Barriers
Protein digestion begins in the stomach and continues through the jejunum.
Enzymes released from:
• The stomach
• The pancreas
• The intestinal brush border
break complex proteins into dipeptides, tripeptides, and free amino acids, which can be absorbed by enterocytes.
However, this enzyme-rich environment also presents a challenge. Many peptides and protein-based bioactives are highly susceptible to enzymatic degradation, which limits their oral bioavailability before absorption can occur.
5. Fat Absorption and Lipid Transport Pathways
Fats and fat-soluble nutrients follow a unique absorption route.
• Lipases break down fats into fatty acids and monoglycerides
• Bile salts emulsify these lipids in the small intestine
• The digested lipids assemble into micelles
These micelles transport lipid molecules across the intestinal lumen to enterocytes, where absorption occurs. Highly lipophilic compounds may also enter the intestinal lymphatic system, allowing them to bypass hepatic first-pass metabolism and improve systemic availability.
6. Key Biological Barriers to Absorption
a. Mucus Layer
The intestinal lining is protected by a mucus layer secreted by goblet cells. While essential for gut protection, this layer:
• Acts as a physical diffusion barrier
• Can limit access of nutrients and bioactives to the epithelial surface
Thick or rapidly renewing mucus can significantly reduce absorption efficiency.
b. Tight Junctions
Hydrophilic nutrients rely on the paracellular pathway for absorption. Tight junction proteins regulate this pathway and act as a size- and charge-selective barrier, limiting the passage of large or polar molecules.
As a result, paracellular transport contributes only minimally to overall absorption.
c. Efflux Transporters
Efflux transporters such as P-glycoprotein (P-gp), MRP, and BCRP actively pump certain compounds back into the intestinal lumen.
These transporters:
• Reduce intracellular accumulation
• Cause site-specific and variable absorption
• Contribute to inter-individual variability in bioavailability
For many compounds, increasing dose alone does not overcome this barrier.
d. Enzymatic Degradation
Digestive enzymes and gut microbiota can degrade nutrients before absorption. While enzymatic activity is essential for digestion, it also:
• Reduces stability of sensitive compounds
• Limits effective absorption
In some cases, enzymatic transformation activates compounds (as seen with prodrugs), but for most nutrients, degradation leads to loss of efficacy.
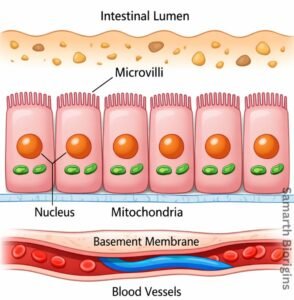
Figure: Structure of the intestinal epithelium showing the lumen, microvilli (brush border), enterocytes, and underlying blood vessels — the primary site of oral nutrient absorption.
7. First-Pass Metabolism
Even after successful intestinal absorption, many compounds undergo first-pass metabolism in the liver.
This metabolic processing can:
• Convert compounds into inactive metabolites
• Significantly reduce systemic availability
Lipophilic compounds that enter lymphatic transport can partially bypass this effect, improving bioavailability.
8. Why Formulation Matters
Because oral absorption is limited by multiple physiological barriers, formulation strategies have evolved to:
• Improve solubility
• Enhance membrane interaction
• Protect against enzymatic degradation
• Reduce efflux and first-pass loss
Advanced delivery systems, including lipid-based and nanocarrier formulations, are designed to work with the body’s natural absorption pathways rather than against them.
Conclusion
Oral nutrient absorption is a complex, multi-step process influenced by digestion, biological barriers, transport mechanisms, and metabolism. Effective absorption depends not only on what is consumed, but on how well the formulation aligns with intestinal physiology.